The fat in your milk accounts for 50% of the calories your baby takes in each feeding. While protein and lactose remain relatively stable throughout the day, milk fat concentration can vary by 47% in a 24 hour period!
Factors that influence milk fat in breast milk: 🤱🏽 In the lactation parent (some of these you can change and control and some of these you can’t): Lifestyle Diet Body size Health or disease/inflammation Number of children Type of birth Overall milk volume produced daily
👶🏼 In the baby (the lactating parents body responds to make specific milk to accommodate the baby): Gender Gestational age Birth weight
🍫 Other factors that influence fat in human milk: ⏰ Time of day (highest fat is in the afternoon/evening) 👶🏼 👧🏽 Stage of lactation (colostrum has the lowest amount of fat. Extended milk for toddlers 12+ months has the highest amount of fat!) 🗓 Time postpartum (milk fat increases with time!) mm Ways to help increase milk fat: 🤱🏽 Feed more frequently. An emptier breast has higher fat and lower water concentrations. Pump ⭐️ Shake your breasts prior to feeding. This gets the fat at the back of the breast to be activated more quickly to flow sooner in the feeding 🐠 Add in healthy fats to your diet: salmon, herring, sardines, flax and chia seeds, and walnuts are high in healthy fats that can boost your milk fat. 🍦 Manage diabetes/blood sugars 🏋🏽♀️ Make sure you’re not anemic or iron deficient ♨️Reduce inflammation in the body (can often be done with diet and lifestyle changes and/or with the help of a naturopathic practitioner)
Your milk can be a variety of colors which can be caused by a variety of things.
💛Diets high in yellow-orange vegetables (yams, squash, carrots, etc) can lead to high levels of carotene in your milk, which can turn it yellow or orange.
💛Frozen milk may look more yellowish when thawed.
🧡Food dyes used in carbonated sodas, fruit drinks, and gelatin desserts have been associated with milk that is pink or pinkish orange.
💙Blueish milk is often just a higher water content in the milk. It could also be caused by food dyes.
💚Greenish milk has been linked to consuming green sports beverages, seaweed, certain herbs, or large amounts of green vegetables (such as kale or spinach). I had mine turn green from a plant based multivitamin!!
💗Pink milk, some times called “strawberry milk” be a sign of blood in your milk. This can occur with or without cracked nipples. Seeing blood in your milk may be alarming at first, but it is not harmful to babies. If you have any concerns or other symptoms associated, such as pain or mastitis, set up a lactation consultation right away.
💔Occasionally blood in breastmilk is caused by things other than nipple or breast trauma. Papillomas are small growths in the milk ducts which are not harmful but can cause blood to enter your milk. In the vast majority of cases, blood in human milk is not a concern. However, some forms of breast cancer can cause blood to leak from the nipples. Breast milk can also turn pink if a bacteria called Serratia marcescens is present, although rare this bacteria can be extremely harmful to young babies. If you’re experiencing pink milk without noticeable nipple damage, please reach out to a health care provider immediately.
🤎Brown milk may be caused by what is known as rusty pipe syndrome. During pregnancy and in the first few days after birth the ducts and milk making cells in your breasts grow and stretch. As blood flows to your breasts it can sometimes leak into your milk ducts, making your milk look brown or rust-colored. It usually clears within a few days as more milk flows through your breasts. Continue feeding your baby your milk.
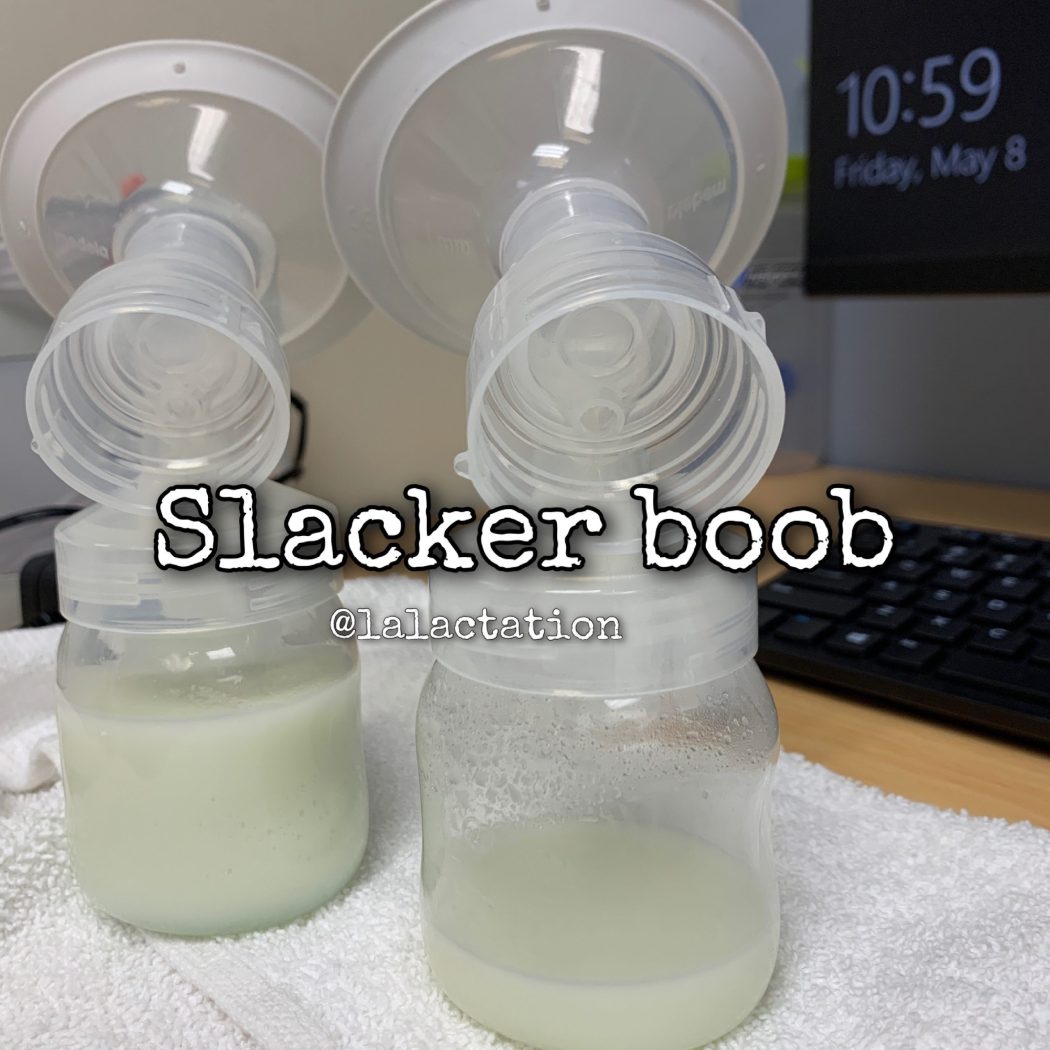
Did you know? Around 70% of women produce more milk in the right breast. Which means 30% make more in the left. It is VERY common for one side to produce more than the other. Some times double on one side. We don’t know why. This is not a reason to neglect one side. You want to make sure you rotate which breast you offer first. Babies may prefer one side over the other for various reasons:
👶🏽They like to lay with their head in a certain direction or their body is uncomfortable in the opposite position
👶🏿They prefer the flow (one side may flow faster or slower than the other)
👶🏼They may prefer the flavor (YES!! Milk can taste different form each breast during the same feeding!!)
If you want to help balance out a slacker boob:
🔆Offer the slacker first more often.
🔆End on the slacker can also help, especially if baby just wants to use you like a pacifier.
🔆Pump the slacker side during or after feedings can also help stimulate more milk production
🔆Make sure you have the correct sized pump flange on the slacker side. Our nipples can often be different sizes and using the wrong sized flange can drop supply on that side
🔆Hand expression on that side at random times of the day even for a few minutes will jump start increased production.
🔆If it’s positional from your baby (they only want to lay cross cradle to the right and not the left, experiment with other positions like football or side lying to help baby compensate for their body. If your baby prefers one side of the other from a positional perspective, consider taking your baby for some infant bodywork like chiropractic or craniosacral therapy.
Breastfeeding going well and all of a sudden you feel like your milk is gone? Go pee on a stick. A drastic drop in milk supply when breastfeeding has been going well can be a sign of pregnancy, even if your period hasn’t come back yet. Research shows it is safe to continue breastfeeding while pregnant and does not increase the risk of miscarriage. So there no reason to wean unless you’re a high risk pregnancy (if you are told by your health care provider that you can’t have sex, you shouldn’t breastfeed. If it’s safe to have sex, it’s safe to continue breastfeeding.) If so you are not alone—far from it.
Key points to remember when breastfeeding and pregnant:
• Milk will shift from mature milk back to colostrum around 14-20 weeks of your pregnancy to prepare for the birth. Babies under 6 months may not get enough milk from the breast alone while toddler eating solids may do fine. Monitor weight gain for babies under 1 year
• Colostrum is saltier than mature milk. Some nurslings are fine with the taste shift and others may self wean
• Aim for a total of about 600 to 800 extra calories — 300 for the fetus and 300 to 500 for milk production.
• Nipples may become extremely tender during pregnancy, especially at the beginning, due to hormone changes
• Breastfeeding aversion while pregnant is normal (feelings of stress or anxiety or wanting to stop breastfeeding)
• If your toddler always nurses to sleep, you may want to find other sleep routines to make putting older one to sleep easier when you have the new baby.
• As your belly grows, you may need to experiment with new breastfeeding positions.
Colostrum is thick and sticky. Pumps are great for stimulating milk but they’re not the best at removing it from the breast and it can be very frustrating to pump and not see anything filling the bottles. Don’t be discouraged. Stimulation is super important in the early days after birth and the work will pay off. hand expression is the key to emptying colostrum when pumping. The pump will do a good job to stimulate your hormones to make milk and your hands will help empty it.
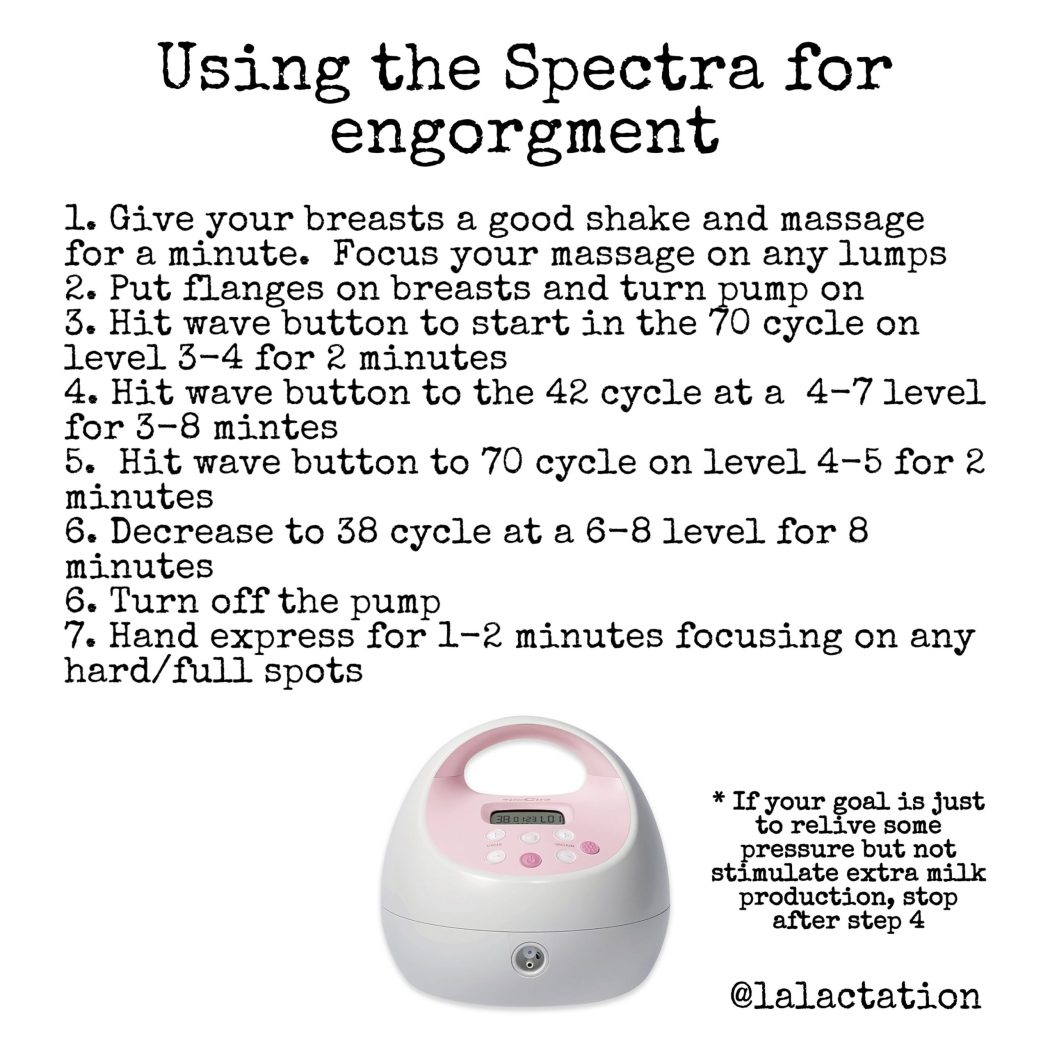
If you’re engorged or have an oversupply, you may need to pump to relieve the pressure in your breasts. Using the pump wisely can reduce your engorgment while not causing you to make too much milk and perpetuate your problem.
You can also pump to increase milk supply by pumping for an extra 5 minutes after milk stops flowing to signal to your body that it needs to produce more milk. If you’re breastfeeding and pumping after, aim for a 10-15 minute pump. If you’re exclusively pumping, shoot for a 30 minute pump.
Whether you’re pumping at work to maintain supply or trying to increase your supply, using the settings on the Spectra can help you reach your goals. Have you played around with your settings? What works for one person may not work for another. Try alternating back and forth between the settings and play around with the suction and cycle levels. If you need to have the suction cranked to the top, you’re most likely using too large of a flange.
Everyone responds differently to pumps. Play around the settings and cycles. What works for one person may not work for every person. Make sure your suction level is comfortable and you’re using the correct sized flange. If you have to crank the suction all the way up, you’re pumping with a flange that’s too large. Pumping should be comfortable. You should not have pain or damage from pumping. If you have any pain or damage, try a different range size, shape or cushion and try lowering the suction. If you’ve been pumping on a particular set of settings and start to notice a decrease in supply or suction, change the soft pieces of the pump like the duckbill or membranes and the tubing.
There is no right or wrong age, it is completely up to you. Breast milk does not lose nutritional value (ever), so you get to decide how long you want to breastfeed. You also get to decide when you stop and all reasons for wanting to stop are valid. It is OK to wean for your emotional or mental well being and you do not have to justify your choices of how you feed your baby to anyone.
The age of your baby and how quickly you want to wean can play a role in how you wean.
Be prepared that some may experience mood changes and feelings of depression when weaning as your oxytocin and other hormones are dropping to stop milk production. If you need a specific plan to help you quickly wean, schedule a consultation with me to develop a plan that works for you.
Tips for gentle weaning:
✏️Start when your baby has already naturally started to wean, ex. only a quick snack before nap or waking up at 2am to pacify to sleep
✏️If transitioning from breast milk to formula, you can add formula to your breast milk bottles in slowly increasing amounts to make the transition easier on baby’s tummy (ex mix 2oz of breast milk with 1oz of prepared formula for several days, then mix 1.5oz each if breast milk and formula for a few days, then 2oz of formula with 1oz of breast milk)
✏️Don’t offer, don’t refuse
✏️Wear clothing that makes accessing the breast/chest more difficult.
✏️Distract child with favorite activities or offer alternatives like a favorite snack
✏️Change your routine
✏️Postpone: “After we play”
✏️Shortening the length of feeding or space feedings out
✏️Talk to your toddler about weaning. Older children (2 years and up) can be part of the process by talking to them about what is happening.
✏️Alternate between offering bottles and the breast
✏️Be consistent – this is a hard one but it can be even more confusing to your baby if you allow them to nurse one time and not the next.
✏️Lots of cuddles. Your breast/chest is more than just food but also a great source of comfort. Showing them you are still a source of that comfort despite not nursing is incredibly important
Ways to quickly wean:
⚓️Empty the breast only to comfort, trying not to stimulate the breast to make more milk
⚓️Breast gymnastics/“milk shakes” often to keep milk from sitting in the breast and clogging the ducts
⚓️Epsom salt soaks of the entire breast for soothing
⚓️Drinking 2-4 cups of sage or peppermint tea per day
⚓️Green cabbage leaves in the bra until they are soggy and then replacing the leaves
⚓️Cabocream (an alternative to the cabbage leaves
⚓️Cold packs on the breasts after feeding or pumping to reduce swelling
⚓️Starting on a hormone based birth control, especially The Pill (estrogen based) will drop supply
⚓️A last resort would be to take an antihistamine like Benadryl or Claritin-D as these are also notorious for dropping milk supply. This should be done with caution and under the direction of your primary care physician
True SELF-weaning by the baby before a year old is very uncommon. In fact, it is unusual for a baby to wean before 18-24 months unless something else going on (work, inefficient feeding, tongue tie, etc). A self weaning child is typically well over a year old (more commonly over 2 years) and getting most nutrition from solids, drinking well from a cup, and has been cutting back on nursing gradually.
Reasons a baby under a year may be perceived to self wean:
🔑Solids were introduced too soon
🔑Scheduled feedings/sleep training/pacifier use (all decrease time a baby would naturally want to be at the breast/chest)
🔑Lactating parent loses a lot of weight fast which can decrease milk supply
🔑Medications or hormonal birth control which will decrease supply
🔑Lactating parent is pregnant
🔑Baby taking lots of solids before one (human milk should be the primary nutrition source through one year of age)
While it seems counterintuitive, the emptier your breasts are, the faster they make milk. A full bread has no place to store or hold the milk, so milk production slows to prevent plugged ducts and breast discomfort. Cluster feeding on an emptier breast actually tells the body to make more milk at a faster rate!! Some incorrectly assume you have to wait for the breast to “fill up” before feeding your baby or for pumping while at work. This will eventually lead to less milk, as a fuller breast tells your body baby isn’t eating very often and to slow milk production. The more frequent you empty the breast, the higher the fat content in that milk and the faster milk is made. The longer often you wait and the fuller the breast, the higher the water content in that milk and the slower your body will make milk overall.
W atch the baby, not the clock. Breasts may feel really full between feedings in the first few weeks after birth, but they’re also not supposed to stay engorged. There will come a time when they stay soft and don’t feel full between feedings or pumping, so waiting for that as a cue to feed will also sabotage your supply. Don’t be alarmed when your breasts no longer feel full between feeding. You’re entering a new stage where you’ll still make plenty of milk for your baby as long as you’re routinely emptying that milk. Trust your body. Trust your baby.
My baby won’t take the breast and is completely refusing to eat. What do I do? I see cases like these occasionally and I feel like they’re some of my most challenging (and most rewarding) cases. If your infant under 6 months is displaying aversion to feeding, we need to figure out why. Aversion to feeding means screaming or crying when even offered the breast, taking very little from the breast, refusing to eat, or needing to be fed while moving or while drowsy/asleep. This is not a temporary nursing strike where baby refuses the breast/bottle for a few days because of periods returning, mom going back to work, teething, or illness, etc. A nursing strike that isn’t managed well can turn into a feeding aversion, though. The behaviors seen in baby are much more extreme for a true aversion. Here is my list of the most common culprits to a true breast aversion in order of most common cause in my experience.
👅Tongue tie/oral motor: Is there a visible tongue or lip tie? One of my biggest red flags for tongue tie is reflux and shutting down during breastfeeding (sleepy baby on the breast, popping on and off, refusing the breast and preferring the bottle but then shutting down on the bottle). Some babies with tongue or lip tie do fine for the first few months as they’re compensating from a full milk supply. The aversion comes around 3-4 months when moms supply regulates and is dictated by the efficiency and responsibility of baby removing milk from the breast. If there is no tie, what’s the baby’s sucking pattern like? Do they have an immature or disorganized suck? How is their latch? Are they possibly taking in too much air with poor latch causing discomfort? Would a different bottle nipple shape or pacing be more appropriate? Do they struggle at the breast but take a bottle occasionally? Address the ties and do oral motor exercises to strengthen and coordinate the system and the refusal goes away.
🥛Intolerances/Allergy: This can look similar to reflux, but there is often a component of bowel issues involved as well (constipation with uncomfortable bowel movements, diarrhea, or mucousy/foamy poops). Look for patterns with formula changes- sometimes parents will say one formula works better than another, and if we look at the formula ingredients we might understand which ingredients baby is sensitive to. Babies who’s digestive tracts are uncomfortable don’t want to eat. They learn really quickly to associate feeding with pain, so they shut down on feeding. Finding the allergens clears the gut and makes feeding pleasant again.
🤮Reflux: Easiest culprit to blame and mask with medication. To be honest, putting baby on reflux meds rarely makes a difference. The medication may mask the pain but won’t actually take the reflux away. Don’t get me wrong, for some babies it can make a big difference, but let’s get to the root of the reflux. And medications should always be a last resort. Is the baby spitting up (doesn’t always happen with reflux)? Is there pain associated with the spit up? Is it projectile and frequent? Does the refusal stop once the bottle is removed or are there signs of discomfort even after the bottle is removed? Wanting small, frequent feedings is my classic tell tale of reflux. Continually swallowing helps keep acid in the stomach and reduces the pain. True reflux is usually caused by food allergy/intolerance, gut issues, or tongue tie. Address the issue, resolve the reflux.
🥵Aspiration: Milk going into the lungs instead of to the stomach. Is the baby stressed during feeding? Do their nostrils flare and their body get stiff or arch? Do the cough and choke throughout the feeding and not just during let down? Do they have noising breathing or feeding? Do you need to be super careful with position change/flow rate changes? Do they have a respiratory history (not just pneumonia- does the baby take long periods to get over any illness)? Further assessment by a speech pathologist is always needed.
🤯Behavioral: I’m not sure if “behavioral” is the correct word, but it’s the best way to describe it. The number one concern of parents is feeding the baby. When feeding isn’t going well, it causes extreme stress, which can cause us as parents to do extreme things to try to fix the problem. It’s easy to spiral out when you’ve tried everything and it’s not working out of stress and desperation (or not being able to figure out the why in the first place). Occasionally the reason for the refusal is not longer there, but it was so stressful in the moment, the panic that it could happen again sets in and perpetuates the problem unnecessarily. Some times the root issue is still there, but you’ve compensated and it’s causing a behavioral manifestation in both you and the baby. Are you just trying to push past baby’s stress signs due to your own stress with trying to get baby fed? Are you just trying a bunch of different things to see what works? Are you trying to feed based off of old information? You are just trying to do your best and are scared for baby, but sometimes the compensatory things we do can cause more problems or cause it to persist. Having an outside observer come in to help see what’s going on can help bring everyone back to baseline.
When trying to figure out which of these culprits is the cause of the aversion, know that you don’t have to figure it out alone. Finding a trained lactation consultant (🙋🏽♀️) can help ask the right questions to get to the root of the issue and get feeding back on track.
We come in all different shapes and sizes, and so do our breasts/chests. They can be large, petite, round, tubular, wide, narrow, symmetrical, uneven, teardrop shaped, or droopy. All of these types of breasts/chest are normal.
The size of your breasts/chest is based upon the amount of fatty tissue in it. Those with smaller breasts have less fatty tissue, and those with larger breasts have more fatty tissue. The fatty tissue doesn’t make breast milk. Glandular tissue inside the fatty tissue produces the breast milk.
Unlike fat, the amount of milk-making tissue in your breasts is not necessarily related to the size of your breasts. People with all different breast sizes are fully capable of producing a healthy supply of breast milk for their babies.
Smaller breasts does not necessarily mean smaller milk supply. As long as the small size is not related to hypoplastic breasts (not enough glandular tissue), there shouldn’t be an issue. While you may have to breastfeed more often due to the amount of breast milk that your breasts can hold, you can still successfully produce enough milk.
Breastfeeding with large breasts has its own unique challenges, usually related to position and how to hold or support the breast. Side lying or rolling a towel to put underneath the breast to lift it can be very helpful. Some worry that their breasts will block baby’s nose. Pulling baby in the opposite direction of the breast and compressing the breast from the back can help pop baby’s nose up off the breast. If your baby’s nose gets blocked while nursing, they will open their mouth and let go of the breast so they can breathe.
If you were told your breasts were too big or too small to breastfeed, I am so sorry. Your body is perfect just the way it is.
If you’re concerned that you’re not producing enough milk, pay attention to your baby’s wet diapers and bowel movements. Generally, small infrequent bowel movements or less than six wet diapers a day, are cause for concern. Contact a lactation consultant (🙋🏽♀️)right away.
Did you know that many of us will notice a supply drop right before our period is going to start and lasts through the period? This is caused by hormone shifts in your body. As supply dips, the milk flow slows. Research shows that the composition of breast milk changes around ovulation (mid-cycle). The levels of sodium and chloride in the milk go up while lactose (milk sugar) and potassium go down. So, the breast milk becomes saltier and less sweet during this time. Some babies become frustrated with this change. They may grab the nipple with their mouth and shake their head back and forth. Pop on and off the breast. Knead or beat the breast with their hands or become extra fussy at the breast. They may even cluster feed and act as if they’re still hungry. They’re trying all the strategies to get your milk to flow how they prefer.
Also around the time of ovulation and just before the start of your period, estrogen and progesterone levels change which can affect your breasts and your breast milk. When estrogen and progesterone levels go up, it can make your breasts feel full and tender.
Higher estrogen levels can also interfere with milk production. Studies also show that calcium levels in the blood go down after ovulation. The lower level of calcium may also contribute to the drop in the milk supply. Lower levels of calcium may also cause your nipples to feel sore, making breastfeeding during your period uncomfortable or sometimes painful.
This is a temporary dip but can be surprising the first time it happens. Remember: this dip can happen once or twice before you actually have a period as your hormones are shifting back into baby making mode. If your baby is older than 6 months and eating lots of solids, you may not notice a difference. The strongest behaviors are seen under 6 months when babies need an exclusive milk diet. You may also notice the dip if you’re a pumper.
Having your period start again may not have any effect on your baby or your milk supply. Some babies continue to breastfeed well. Others will not like the taste of the breast milk or the drop in the amount of breast milk that can happen when your period returns. Your baby may:
Become fussier than normal
Want to breastfeed more due to the lower milk supply
Breastfeed less because there is less breast milk and it tastes different
Nursing strike
What can you do about it? Knowing it can happen is the first step. Stay well hydrated and eat quality nutrition. Many find adding in a calcium/magnesium supplement (1000mg of calcium/500mg magnesium per day split into 3-4 “doses”) can help combat the drop. Others find adding in lactation specific herbs or supportive foods help. Iron rich foods like dark leafy greens and red meat and milk making foods like oatmeal, almonds and fennel can really help. Keep offering the breast or pumping frequently. It will get better and your supply will come back up as soon as your hormones shift again after your period. It usually only lasts a few days.
Word to the wise: You can release an egg from your ovary (ovulate) before your period returns. If you’re involved in an intimate relationship, and you’re not using birth control, you can get pregnant again without ever getting your first period even while you’re breastfeeding. If you notice a very drastic drop in milk supply, consider taking a pregnancy test.