Your milk can be a variety of colors which can be caused by a variety of things.
💛Diets high in yellow-orange vegetables (yams, squash, carrots, etc) can lead to high levels of carotene in your milk, which can turn it yellow or orange.
💛Frozen milk may look more yellowish when thawed.
🧡Food dyes used in carbonated sodas, fruit drinks, and gelatin desserts have been associated with milk that is pink or pinkish orange.
💙Blueish milk is often just a higher water content in the milk. It could also be caused by food dyes.
💚Greenish milk has been linked to consuming green sports beverages, seaweed, certain herbs, or large amounts of green vegetables (such as kale or spinach). I had mine turn green from a plant based multivitamin!!
💗Pink milk, some times called “strawberry milk” be a sign of blood in your milk. This can occur with or without cracked nipples. Seeing blood in your milk may be alarming at first, but it is not harmful to babies. If you have any concerns or other symptoms associated, such as pain or mastitis, set up a lactation consultation right away.
💔Occasionally blood in breastmilk is caused by things other than nipple or breast trauma. Papillomas are small growths in the milk ducts which are not harmful but can cause blood to enter your milk. In the vast majority of cases, blood in human milk is not a concern. However, some forms of breast cancer can cause blood to leak from the nipples. Breast milk can also turn pink if a bacteria called Serratia marcescens is present, although rare this bacteria can be extremely harmful to young babies. If you’re experiencing pink milk without noticeable nipple damage, please reach out to a health care provider immediately.
🤎Brown milk may be caused by what is known as rusty pipe syndrome. During pregnancy and in the first few days after birth the ducts and milk making cells in your breasts grow and stretch. As blood flows to your breasts it can sometimes leak into your milk ducts, making your milk look brown or rust-colored. It usually clears within a few days as more milk flows through your breasts. Continue feeding your baby your milk.
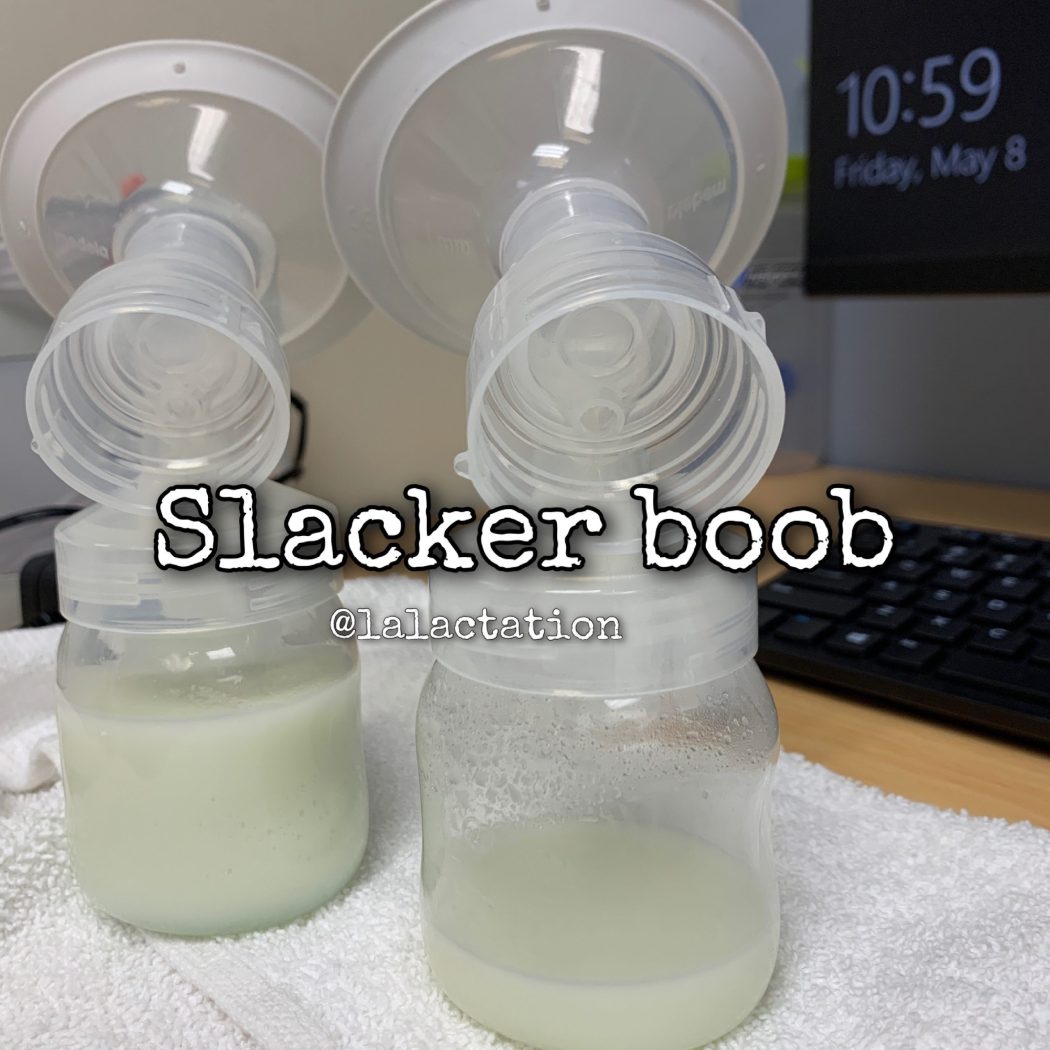
Did you know? Around 70% of women produce more milk in the right breast. Which means 30% make more in the left. It is VERY common for one side to produce more than the other. Some times double on one side. We don’t know why. This is not a reason to neglect one side. You want to make sure you rotate which breast you offer first. Babies may prefer one side over the other for various reasons:
👶🏽They like to lay with their head in a certain direction or their body is uncomfortable in the opposite position
👶🏿They prefer the flow (one side may flow faster or slower than the other)
👶🏼They may prefer the flavor (YES!! Milk can taste different form each breast during the same feeding!!)
If you want to help balance out a slacker boob:
🔆Offer the slacker first more often.
🔆End on the slacker can also help, especially if baby just wants to use you like a pacifier.
🔆Pump the slacker side during or after feedings can also help stimulate more milk production
🔆Make sure you have the correct sized pump flange on the slacker side. Our nipples can often be different sizes and using the wrong sized flange can drop supply on that side
🔆Hand expression on that side at random times of the day even for a few minutes will jump start increased production.
🔆If it’s positional from your baby (they only want to lay cross cradle to the right and not the left, experiment with other positions like football or side lying to help baby compensate for their body. If your baby prefers one side of the other from a positional perspective, consider taking your baby for some infant bodywork like chiropractic or craniosacral therapy.
Colostrum is thick and sticky. Pumps are great for stimulating milk but they’re not the best at removing it from the breast and it can be very frustrating to pump and not see anything filling the bottles. Don’t be discouraged. Stimulation is super important in the early days after birth and the work will pay off. hand expression is the key to emptying colostrum when pumping. The pump will do a good job to stimulate your hormones to make milk and your hands will help empty it.
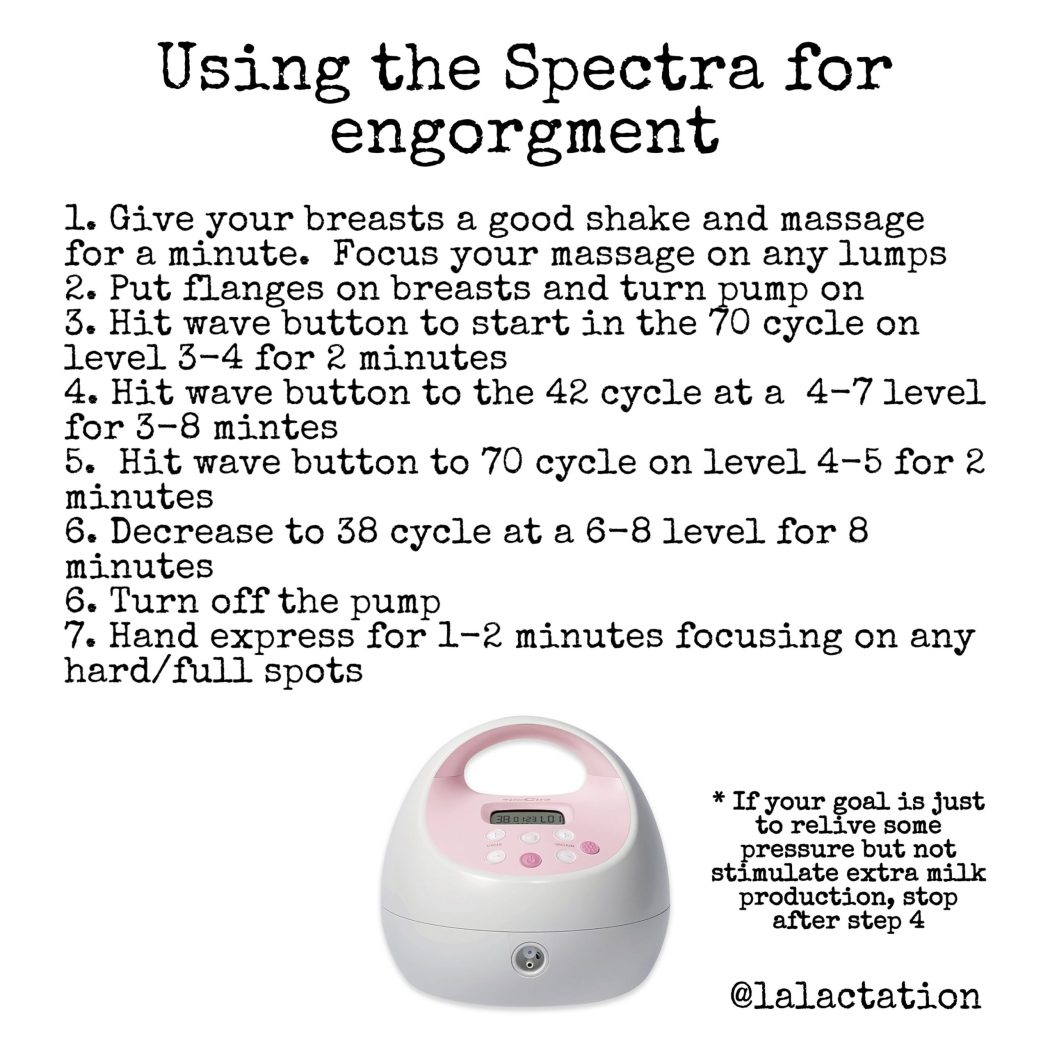
If you’re engorged or have an oversupply, you may need to pump to relieve the pressure in your breasts. Using the pump wisely can reduce your engorgment while not causing you to make too much milk and perpetuate your problem.
You can also pump to increase milk supply by pumping for an extra 5 minutes after milk stops flowing to signal to your body that it needs to produce more milk. If you’re breastfeeding and pumping after, aim for a 10-15 minute pump. If you’re exclusively pumping, shoot for a 30 minute pump.
Whether you’re pumping at work to maintain supply or trying to increase your supply, using the settings on the Spectra can help you reach your goals. Have you played around with your settings? What works for one person may not work for another. Try alternating back and forth between the settings and play around with the suction and cycle levels. If you need to have the suction cranked to the top, you’re most likely using too large of a flange.
Everyone responds differently to pumps. Play around the settings and cycles. What works for one person may not work for every person. Make sure your suction level is comfortable and you’re using the correct sized flange. If you have to crank the suction all the way up, you’re pumping with a flange that’s too large. Pumping should be comfortable. You should not have pain or damage from pumping. If you have any pain or damage, try a different range size, shape or cushion and try lowering the suction. If you’ve been pumping on a particular set of settings and start to notice a decrease in supply or suction, change the soft pieces of the pump like the duckbill or membranes and the tubing.
Did you know babies routinely get antibodies to anything you’ve been vaccinate against? Babies get temporary disease protection from you in this way. When you are vaccinated, your body has an immune response that makes antibodies to what you were vaccinated against. Antibodies are then secreted in breast milk to your baby. The type and quantity of these antibodies, and whether they provide any protection for baby after they are swallowed, are dependent on the vaccine received and maternal factors that influence immune system function such as genes, age and health.
Antibodies in breast milk have not been shown to reduce baby’s response to their own immunizations. However, some studies suggest that breast milk may improve baby’s immune response to some of the vaccines they receive.
If you do decide to be vaccinated while breastfeeding, there is no need to pump and dump your milk. Or to stop breastfeeding for any amount of time. When considering the vaccine, or any medication, most want to know whether a dangerous amount of a substance will be filtered into our milk and cause harm to our baby. For most drugs, so little gets to the baby that there’s really very little theoretical risk. Even if a drug or vaccine does end up in breastmilk, anything that goes through breastmilk also then has to go through baby’s gut before reaching baby’s bloodstream. The mRNA molecules in the Pfizer or Moderna vaccines, if they made it into your milk, would have to survive baby’s stomach acid first.
While breastfeeding, it is highly unlikely that an intact lipid from the vaccine would enter your blood stream and be passed directly into your milk. If it does, it is even less likely that either the intact nanoparticle or mRNA could be transferred into your milk. In the unlikely event that mRNA is present in your milk, it would first go through baby’s digestive system and would be unlikely to have any biological effects. The vaccine is supposed to trigger an immune response in your body. It helps your body recognize the virus when you’re exposed and fights the virus early, reducing the severity and length of illness. Once your immune system recognizes the SARS-CoV-2, the virus that causes Covid-19, antibodies are made to protect you and those antibodies may pass into the breastmilk. Researchers have already found Covid antibodies in the breastmilk of previously infected women, though they don’t know yet how much protection these antibodies give babies.
Choosing to be vaccinated is a personal risk/benefit decision to be made between you and your health care providers. If you do chose to be vaccinated with the COVID vaccines, there is no need to pump and dump for concerns of your milk harming your baby.
What pump do you have? What size flange are you using? The answer can make a huge difference in pumping success.
Not all pumps are created equal. Prior to the ACA, there were few pump choices. Once laws said people needed to be provided with a breast pump, and insurance would fit the bill, lots of companies flooded the market with pumps. Not all of them are good, and some will even sabotage your supply. You want a pump with a good motor in it that has lots of variability in the cycle (how fast or slow it pumps) and suction (how strong it sucks).
You also need to be mindful of the flange you’re pumping on. Most companies will send a standard 24mm flange. Sometimes they’ll send a larger size as well. In reality nipples, and thus flanges, are not one size fits all. And in my practice I hardly EVER use the 24 or bigger flanges. For almost all of my families we’re sizing down. Some times significantly smaller.
Flanges are the horn shaped part that actually touch the breast. The fit of the flange can make or break your pumping experience. Too small and friction can cause pain and even damage (and pain makes it difficult for milk to let down). Too large and the breast may not be stimulated well, which inhibits your let down to have milk flow. When too much areola is pulled into the flange, the tissue swells around the nipple pores and can prevent milk from efficiently emptying from the breast, resulting in plugged ducts, pain, tissue breakdown, and eventually a reduced milk supply. Using too large of a flange from the beginning may even prevent you from bringing in a full milk supply. Do you ever pump for 20+ minutes and still feel like there’s milk in there? Most likely too large of a flange. The stimulation from the pump is triggering you to make more milk, but the size of the flange is preventing you from emptying that milk efficiently. Poor flange fit can also impact the suction of your pump and how well it functions with your body. If you have the suction all the way to the highest level and aren’t emptying well, you flange is too big.
Flange fit tips:
Some of the flanges I tried
🗝Flange fit isn’t based on your breast or areola size, it is JUST the size of the nipple and how it changes with suction. Some nipples are dense and don’t stretch much. Some are super elastic and swell a lot. How your nipple responds to suction can make a difference in which flange you select and if other products are needed to happy pump
🗝Proper fit isn’t as simple as measuring your nipple, but it’s a start. See a trained IBCLC to help if you haven’t found the right fit or are struggling with poor output, pain/damage, or plugged ducts
🗝A small amount of space around your nipple in the flange tunnel is good. There should be no space around the areola or in the larger bell part of the flange. If your breast tissue recoils back into the horn part of the flange with every cycle, the flange is too large. If the tissue is white where the tunnel meets the horn, the flange is too small
🗝Pain or blanching means it’s the wrong size
🗝Nipples rubbing against the sides of the flange tunnel mean fit needs to be improved and there is a risk of pain and damage
🗝There should only be a small amount of areola pulled in the flange tunnel space. The bell or horn part will have most of the areola held back so it doesn’t get pulled into the tunnel
🗝The nipple tip shouldn’t hit the back of the flange. This means you have an elastic nipple. Sizing up isn’t necessarily the right answer. Using a pump insert, cushion like @beaugenmom or @pumpinpalofficial may be a better solution
🗝Evaluate as you pump. You can changing flange size mid-pump to improve comfort if you’re between sizes. You may also need to change the flange size the longer you pump. Our nipples can become more elastic and larger or smaller with time.
🗝Every nipple is unique and each side may use a different size (or shape/brand!). There are all kinds of flange sizes, inserts, and cushions to improve the pump experience
If breastfeeding is going well and you’re planning on being home with your baby or only gone for a few hours at a time there is no need to have a huge freezer stash. Having milk in the freezer is a nice security, especially is your have to work or will be away from your baby. But if you’re always with your baby or are only gone for a short while, there is no need to have a stash.
Having the right stash for your family means having enough stashed for when you’re away from your baby. If you’re gone for one feeding, you only need one feeding worth of milk. If you’re gone 2-3 feedings, you need 2-3 feedings worth of milk. If your baby is being bottle feeding while you’re away, you would pump while you’re gone to tell your body the milk is needed. That milk then becomes the stash for the next time that you’re gone.
If you want to have a big stash, great!!! You can absolutely have that as an option. Just don’t feel pressured from other people’s journeys on social media to have something you may not need or use. I’ve had several moms who spent countless hours pumping and stashing only to have to donate or throw out the milk stash because they never used it and it was going to expire. I’ve also had several moms who thought you had to have a stash and were relieved to know they didn’t! Do what is best for you and your baby and not based off of anyone else.
You’ve got this. Trust your body. Trust your baby.
While your young baby is supposed to gain on average an ounce a day (30gm), weight gain slows as baby ages. From 4-6 months babies should only gain 3-4 ounces per week (90-120gm) and from 6-12 months babies should only gain 1-2 ounces per week (30-60gm). If you have been tracking baby’s weight gain and see the scale slowing down, don’t be alarmed if your baby is older. Continue to watch for lots of wet diapers and consistent pooping. Trust your baby and trust your body.
An IUD is a form of birth control that’s put into your uterus to prevent pregnancy. One of the most common forms of birth control, it’s long-term, reversible, and considered one of the most effective birth control methods. Many doctors will encourage new mothers to have them placed between 4-6 weeks postpartum checkup to prevent pregnancies too close together. The Paragard IUD is wrapped in copper and doesn’t have hormones. The Mirena, Kyleena, Liletta, and Skyla IUDs use the hormone progestin to prevent pregnancy. Be aware that each IUD has a different amount of progestin. They are not created equal. Progestin is also the hormone found in the mini pill.
Hormonal IUDs and the mini pill are often recommended by doctors as the best form of birth control for breastfeeding mothers because most of the research that is available says that they don’t impact breast milk supply. And many who use these methods don’t experience any drop in supply. For some, though, both the mini pill and the hormonal IUDs will drop breast milk supply, some times drastically. Every body is sensitive to different levels of hormones. If you have an IUD placed and notice a drop in supply, the only way to increase supply again is to remove the IUD. Increased pumping or herbal supplements will usually not be enough to increase supply again because you’re working against hormones. The only way to rebound supply would be to remove the IUD. If you’re considering a hormonal based IUD and aren’t sure if your supply will drop, consider taking a few rounds of the mini pill (progestin only) which is the same hormone as the IUD. If your supply drops, you only have to stop taking the pill and your supply will rebound much quicker.
Did you use a hormone based birth control? Did you notice a change in your breast milk supply?
For the first six months after birth, baby is supposed to be on an exclusive breast milk diet. At six months and beyond your breast milk goes through a major change. The volume of milk slowly drops because baby is eating and drinking other foods. They may also be sleeping longer at night and are more active during the day. Your milk is super smart and shifts with this drop to have more antibodies and a higher fat content. The breast makes milk based on how it is emptied and what your hormones are doing based on how old baby is. Your hormones are also shifting and you may start your monthly cycle again. Many experience a further dip in supply around the time with their period. If you’re exclusively breastfeeding, you may notice baby pulling or tugging on your nipple or using their hands to beat your chest while feeding. If you’re pumping, you may slowly start to see less milk each pump session. Usually months 5-7 are the hardest from a baby behavior perspective and it settles out again as baby eats more table food and your hormones adjust. If breastfeeding is your goal, just keep offering the breast and pumping often.
It is normal for let-down not to feel as strong as baby gets older. Some of us never feel let-down, and some stop feeling the let-down sensation as time goes by. This does not necessarily indicate that let-down is not taking place. Remember, just because you don’t feel it or it feels different over time, or any mean it’s not happening.
Signs of let-down include:
• Uterine cramping during letdown in the first week postpartum
• Baby’s sucking pattern changes from a quick suck-suck to a rhythmic suck-swallow pattern as milk begins to flow
• Feeling of calm, relaxation, sleepiness or drowsiness.
• Sudden thirst
• Leaking from the other breast
• Tingling, pins and needles sensation, itching, nausea, headaches, or negative emotions
Things that can be the cause of a slow or inhibited let-down:
• History of breast surgery where nerve damage that can interfere with let-down.
• In extreme situations of stress or crisis, the release of extra adrenaline in can reduce or block the hormones which affect let-down from a fight or flight response
• Sometimes a cycle is created, where baby fusses and pulls off because the let-down is slow, which makes mom tense up, which makes the let-down even slower, etc.
• It’s normal to have a harder time letting down for the pump than baby.
Later into your breastfeeding journey, you may notice it takes longer to trigger a let-down. This is common and what works early on may change over time.
Check for possible causes:
• Worn pump parts that need replaced. Replace the valves and membranes often. Check for worn tubing.
• Make sure you’re pumping with the correct flange size. Nipples may become more elastic over time and a different size may be used.
• Starting your period or are you possibly pregnant? Both can decrease milk production and impact let-downs.
• New hormonal birth control or medication? These may impact supply.
• Check your body. Tension, pain, cold, fatigued or anxiety may block the neurochemical pathways required for milk let-downs.
Tips to trigger let down:
• Try a different pump or flange size
• Use heat, breast massage/compressions, or vibrations to prompt milk flow
• Orgasm. The same hormone released during orgasm also causes let down. Studies show having an orgasm can help let down
• Relax. Use slow, deep breaths and meditation
• Singing or humming can also speed let-down
• Gently massage your breasts. Stroke your breast towards the nipple with the flat of your hand or edge of a finger. Gently roll your nipple between your fingers
• Watch videos of your baby. Smell their clothing. Remember the feeling of let down
• Use all of your senses to facilitate let-down. Concentrate on the sight, sound, smell and feel of your baby.
• Take a warm shower or bath prior to nursing
• If you are in any pain, consider taking a pain reliever about 30 minutes before you feeding. Pain can cause stress and inhibit let-down.
• Choose a calm, less distracting setting
• Turn on music or a tv show that you enjoy
• Skin to skin contact with your baby: Undress baby to their diaper and yourself from the waist up. Stay like this for 1-2 hours prior to a feeding
• Eat a favorite snack and drink a comforting beverage like warm tea
• Get comfortable. Sit in a comfy chair or lay in bed. You should be in a comfortable position
• Switch nurse: move baby back and forth frequently between breasts until let-down occurs
• Visualization. Take several deep breaths and close your eyes as you begin. Try to visualize and “feel” what the let-down response feels like for you (if you normally feel anything). Imagine milk flowing or use images of waterfalls. An excellent book on visualization techniques is Mind Over Labor by Carl Jones.
• Distraction: watch TV, read, talk to a friend, don’t watch the pump bottles.
• One study has shown that the moms of hospitalized babies who listened to guided relaxation or soothing music while pumping had an increased pumping output. When mom listened to a recording that included both music and guided relaxation while pumping, in addition to looking at photos of her baby, pumping output was increased even more. In this study, the interventions led to moms producing 2-3 times their normal pumping output. Milk fat content also increased for these moms in the early days of the study. (Reference: Keith DR, Weaver BS, Vogel RL. The effect of music-based listening interventions on the volume, fat content, and caloric content of breast milk-produced by mothers of premature and critically ill infants. Adv Neonatal Care. 2012 Apr;12(2):112-9.)