Breasts are made of a network of ducts, covered by a layer of fatty tissue. During pregnancy, estrogen and progesterone enlarge the milk ducts and multiply the glandular tissue that produces milk. After birth, estrogen and progesterone drop and prolactin and oxytocin rise. Prolactin makes milk production and oxytocin releases it into the ducts. Extra blood and fluid fill the breast just after birth to supoort your body adding hormone receptors in the breast to make milk. The blood and fluid surrounds the ducts and this extra pressure is what makes your breasts feel full between feeding. This blood and fluid reabsorb around 6-8 weeks once supply is established and you won’t feel that full/soft feeling except when you go a really long time between feeding or pumping. Breasts go back to prepregnancy size when supply regulates around 11-14 weeks but continue to make milk. When you wean from breastfeeding, it can take several months for prolactin levels to return to baseline (which is why you may still see milk for months after weaning). Once you stop breastfeeding, the milk making structures actually self-destruct – a process that involves massive cellular suicide, and the removal of the debris. Around 6 months after weaning, the milk-producing tissue is replaced with fatty tissue. If you return to your pre-pregnancy weight, your breasts most likely will return to the same size. They may not be as “perky” because the skin is a bit more stretched and the connective and fatty tissues in the breasts often shifts during pregnancy and breastfeeding. While they may look smaller after weaning most of us can expect that our breasts will return to a similar size as they were pre-pregnancy. They’re just a little more lived in and well loved.
Colostrum is thick and sticky. Pumps are great for stimulating milk but they’re not the best at removing it from the breast and it can be very frustrating to pump and not see anything filling the bottles. Don’t be discouraged. Stimulation is super important in the early days after birth and the work will pay off. hand expression is the key to emptying colostrum when pumping. The pump will do a good job to stimulate your hormones to make milk and your hands will help empty it.
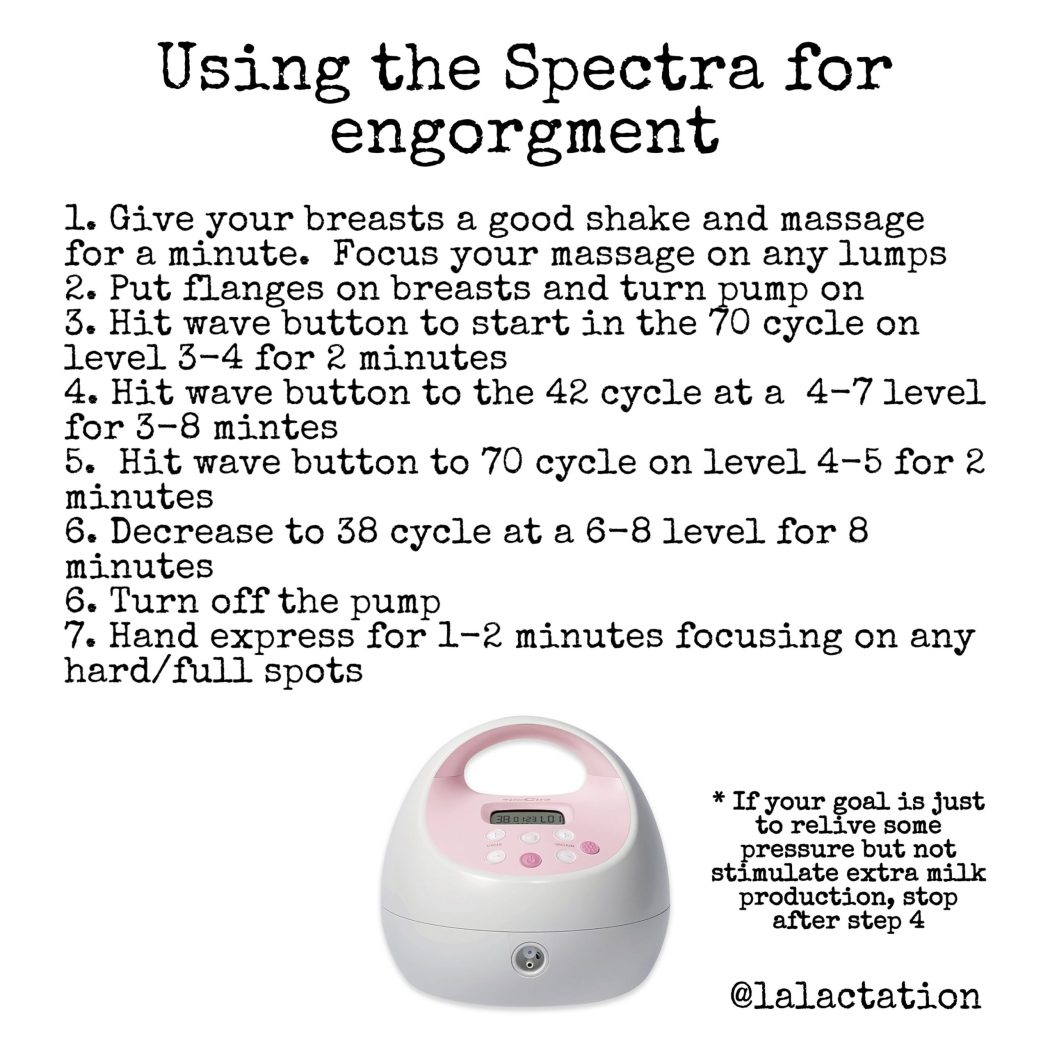
If you’re engorged or have an oversupply, you may need to pump to relieve the pressure in your breasts. Using the pump wisely can reduce your engorgment while not causing you to make too much milk and perpetuate your problem.
You can also pump to increase milk supply by pumping for an extra 5 minutes after milk stops flowing to signal to your body that it needs to produce more milk. If you’re breastfeeding and pumping after, aim for a 10-15 minute pump. If you’re exclusively pumping, shoot for a 30 minute pump.
Whether you’re pumping at work to maintain supply or trying to increase your supply, using the settings on the Spectra can help you reach your goals. Have you played around with your settings? What works for one person may not work for another. Try alternating back and forth between the settings and play around with the suction and cycle levels. If you need to have the suction cranked to the top, you’re most likely using too large of a flange.
Everyone responds differently to pumps. Play around the settings and cycles. What works for one person may not work for every person. Make sure your suction level is comfortable and you’re using the correct sized flange. If you have to crank the suction all the way up, you’re pumping with a flange that’s too large. Pumping should be comfortable. You should not have pain or damage from pumping. If you have any pain or damage, try a different range size, shape or cushion and try lowering the suction. If you’ve been pumping on a particular set of settings and start to notice a decrease in supply or suction, change the soft pieces of the pump like the duckbill or membranes and the tubing.
What pump do you have? What size flange are you using? The answer can make a huge difference in pumping success.
Not all pumps are created equal. Prior to the ACA, there were few pump choices. Once laws said people needed to be provided with a breast pump, and insurance would fit the bill, lots of companies flooded the market with pumps. Not all of them are good, and some will even sabotage your supply. You want a pump with a good motor in it that has lots of variability in the cycle (how fast or slow it pumps) and suction (how strong it sucks).
You also need to be mindful of the flange you’re pumping on. Most companies will send a standard 24mm flange. Sometimes they’ll send a larger size as well. In reality nipples, and thus flanges, are not one size fits all. And in my practice I hardly EVER use the 24 or bigger flanges. For almost all of my families we’re sizing down. Some times significantly smaller.
Flanges are the horn shaped part that actually touch the breast. The fit of the flange can make or break your pumping experience. Too small and friction can cause pain and even damage (and pain makes it difficult for milk to let down). Too large and the breast may not be stimulated well, which inhibits your let down to have milk flow. When too much areola is pulled into the flange, the tissue swells around the nipple pores and can prevent milk from efficiently emptying from the breast, resulting in plugged ducts, pain, tissue breakdown, and eventually a reduced milk supply. Using too large of a flange from the beginning may even prevent you from bringing in a full milk supply. Do you ever pump for 20+ minutes and still feel like there’s milk in there? Most likely too large of a flange. The stimulation from the pump is triggering you to make more milk, but the size of the flange is preventing you from emptying that milk efficiently. Poor flange fit can also impact the suction of your pump and how well it functions with your body. If you have the suction all the way to the highest level and aren’t emptying well, you flange is too big.
Flange fit tips:
Some of the flanges I tried
🗝Flange fit isn’t based on your breast or areola size, it is JUST the size of the nipple and how it changes with suction. Some nipples are dense and don’t stretch much. Some are super elastic and swell a lot. How your nipple responds to suction can make a difference in which flange you select and if other products are needed to happy pump
🗝Proper fit isn’t as simple as measuring your nipple, but it’s a start. See a trained IBCLC to help if you haven’t found the right fit or are struggling with poor output, pain/damage, or plugged ducts
🗝A small amount of space around your nipple in the flange tunnel is good. There should be no space around the areola or in the larger bell part of the flange. If your breast tissue recoils back into the horn part of the flange with every cycle, the flange is too large. If the tissue is white where the tunnel meets the horn, the flange is too small
🗝Pain or blanching means it’s the wrong size
🗝Nipples rubbing against the sides of the flange tunnel mean fit needs to be improved and there is a risk of pain and damage
🗝There should only be a small amount of areola pulled in the flange tunnel space. The bell or horn part will have most of the areola held back so it doesn’t get pulled into the tunnel
🗝The nipple tip shouldn’t hit the back of the flange. This means you have an elastic nipple. Sizing up isn’t necessarily the right answer. Using a pump insert, cushion like @beaugenmom or @pumpinpalofficial may be a better solution
🗝Evaluate as you pump. You can changing flange size mid-pump to improve comfort if you’re between sizes. You may also need to change the flange size the longer you pump. Our nipples can become more elastic and larger or smaller with time.
🗝Every nipple is unique and each side may use a different size (or shape/brand!). There are all kinds of flange sizes, inserts, and cushions to improve the pump experience
It is normal for let-down not to feel as strong as baby gets older. Some of us never feel let-down, and some stop feeling the let-down sensation as time goes by. This does not necessarily indicate that let-down is not taking place. Remember, just because you don’t feel it or it feels different over time, or any mean it’s not happening.
Signs of let-down include:
• Uterine cramping during letdown in the first week postpartum
• Baby’s sucking pattern changes from a quick suck-suck to a rhythmic suck-swallow pattern as milk begins to flow
• Feeling of calm, relaxation, sleepiness or drowsiness.
• Sudden thirst
• Leaking from the other breast
• Tingling, pins and needles sensation, itching, nausea, headaches, or negative emotions
Things that can be the cause of a slow or inhibited let-down:
• History of breast surgery where nerve damage that can interfere with let-down.
• In extreme situations of stress or crisis, the release of extra adrenaline in can reduce or block the hormones which affect let-down from a fight or flight response
• Sometimes a cycle is created, where baby fusses and pulls off because the let-down is slow, which makes mom tense up, which makes the let-down even slower, etc.
• It’s normal to have a harder time letting down for the pump than baby.
Later into your breastfeeding journey, you may notice it takes longer to trigger a let-down. This is common and what works early on may change over time.
Check for possible causes:
• Worn pump parts that need replaced. Replace the valves and membranes often. Check for worn tubing.
• Make sure you’re pumping with the correct flange size. Nipples may become more elastic over time and a different size may be used.
• Starting your period or are you possibly pregnant? Both can decrease milk production and impact let-downs.
• New hormonal birth control or medication? These may impact supply.
• Check your body. Tension, pain, cold, fatigued or anxiety may block the neurochemical pathways required for milk let-downs.
Tips to trigger let down:
• Try a different pump or flange size
• Use heat, breast massage/compressions, or vibrations to prompt milk flow
• Orgasm. The same hormone released during orgasm also causes let down. Studies show having an orgasm can help let down
• Relax. Use slow, deep breaths and meditation
• Singing or humming can also speed let-down
• Gently massage your breasts. Stroke your breast towards the nipple with the flat of your hand or edge of a finger. Gently roll your nipple between your fingers
• Watch videos of your baby. Smell their clothing. Remember the feeling of let down
• Use all of your senses to facilitate let-down. Concentrate on the sight, sound, smell and feel of your baby.
• Take a warm shower or bath prior to nursing
• If you are in any pain, consider taking a pain reliever about 30 minutes before you feeding. Pain can cause stress and inhibit let-down.
• Choose a calm, less distracting setting
• Turn on music or a tv show that you enjoy
• Skin to skin contact with your baby: Undress baby to their diaper and yourself from the waist up. Stay like this for 1-2 hours prior to a feeding
• Eat a favorite snack and drink a comforting beverage like warm tea
• Get comfortable. Sit in a comfy chair or lay in bed. You should be in a comfortable position
• Switch nurse: move baby back and forth frequently between breasts until let-down occurs
• Visualization. Take several deep breaths and close your eyes as you begin. Try to visualize and “feel” what the let-down response feels like for you (if you normally feel anything). Imagine milk flowing or use images of waterfalls. An excellent book on visualization techniques is Mind Over Labor by Carl Jones.
• Distraction: watch TV, read, talk to a friend, don’t watch the pump bottles.
• One study has shown that the moms of hospitalized babies who listened to guided relaxation or soothing music while pumping had an increased pumping output. When mom listened to a recording that included both music and guided relaxation while pumping, in addition to looking at photos of her baby, pumping output was increased even more. In this study, the interventions led to moms producing 2-3 times their normal pumping output. Milk fat content also increased for these moms in the early days of the study. (Reference: Keith DR, Weaver BS, Vogel RL. The effect of music-based listening interventions on the volume, fat content, and caloric content of breast milk-produced by mothers of premature and critically ill infants. Adv Neonatal Care. 2012 Apr;12(2):112-9.)
Paced bottle feeding (meaning you’re setting the pace for how fast/slow baby drinks) helps prevent over feeding baby: it takes 20 minutes for the stomach to tell the brain that it’s full. If a baby takes a bottle too quickly, the mouth can still be “hungry” and wanting to suck when the stomach is actually full. Like going to an all you can eat buffet and eating a lot of food quickly and then realizing half hour later you ate way too much. A baby that happily sucks down too much milk from a bottle can make you think you don’t have enough breast milk even if you make a normal amount. It can also make baby frustrated by the flow of milk from the breast and inadvertently sabotage breastfeeding
These pictures are the same baby in two different positions for paced feeding: semi upright and side lying. Side lying is my favorite position to use as it puts baby in the same position as breastfeeding. Many parents feel baby is more supported in this position. Baby is supported by your leg or breastfeeding pillow.
Tips:
🍼Never feed baby on their back
🍼Keep the bottle parallel with the floor with about half the nipple filled with milk
🍼Use the slowest flow nipple baby will tolerate
🍼Rub the nipple gently on baby’s lips, allow baby to latch at their own pace, don’t force it into their mouth
🍼It should take 15-20 minutes to finish the bottle
🍼Watch the baby and not the bottle, stop when they show signs of being full
🍼Resist the urge to finish the bottle, even if there is only a little left, when baby is showing signs their tummy is full
🍼Take short breaks to burp and give the tummy time to fill naturally
🍼If baby is gulping or chugging, slow down
🍼If baby has taken a good volume of milk (2-4oz) in a short amount of time and is still acting hungry, offer a pacifier for a few minutes to help them digest and give the tummy to to tell the brain it’s full. If they’re still hungry, slowly offer more in 1/2oz increments
How many ounces should I leave if I’m exclusively breastfeeding but need to leave my baby a bottle?
The answer is: that depends. Some babies are grazers. They like smaller, more frequent feedings to keep their tummy from being too full or uncomfortable. Their feedings can range from 1-3 ounces and they may feed 10 or more times a day. Other babies are bingers. They like a big, full tummy and may take 3-5 or even occasionally 6 ounces but not as often. They may feed only 6-8 times a day and have longer sleep stretches. Their tummy doesn’t mind being stretched fuller and their bodies tell them it’s ok to go longer between feedings.
The question is: how many feedings do they get in 24 hours? From one month to one year, babies take between 19-32 ounces of breast milk a day. The average is 25 ounces in 24 hours. There’s a range because babies eat more or less depending on the activities of the day, growth spurts, teething, and even babies emotionally eat sometimes. In general, take 25 and divide it by the number of feedings they average in any given day. Also take into account that growth slows between 6-12 months and baby should be eating table foods, so you don’t need to increase the ounces in the bottle during that time. If your baby took 4 Oz bottles at 4 months, 4 Oz bottles are still appropriate at 9 months because they’re also begging for the food right off your plate in addition to what you’re putting on their tray.
The best way to lose weight is to be in a calorie deficit. Choosing the right foods, protein, fruits and vegetables with moderation of carbs, sugars and starches is guaranteed for most to lose extra pounds. Sure, exercise helps. It helps burn calories, again contributing to calorie deficit. But exercise alone won’t help you lose weight if you’re still eating a high calorie diet. Sure, going vegetarian or vegan or doing Weight Watchers or Atkins or any other “diet” helps. It helps you monitor intake to be in a calorie deficit. But even on any diet plan, if you’re not following it correctly and still eating high amounts of foods you won’t lose weight. Certain people do better on certain diets or with specific exercise programs because of how their specific body handles and processes food, vitamins, stress, movement, and all of the other factors like environment and genetics. Finding a nutritionist, weight loss coach, or personal trainer helps you look at your specific body and goals and helps you reach them. You can absolutely get there in your own, having someone counsel you through often gets you quicker results from their experience and wisdom. But the principle remains: calorie deficit is the number one way to lose weight.
The best way to make breast milk is to empty breast milk. Whether that’s your baby or a high quality breast pump, moving milk multiple times a day tells the body to make more milk. The more often milk is removed, the faster it is made. Sure, supplements help. They support your thyroid and blood with the extra nutrients and hormones needed to produce milk. But supplements alone is no replacement for moving milk. You can take the best lactation bars and drink all the tea you want, but without emptying the breast every few hours routinely I wouldn’t expect the majority of us to make enough milk to feed baby. Sure, hydration and nutrition are important. It takes calories to make calories and hydration help with that process. But even the research shows women who are malnourished in famine torn countries make plenty of milk for their babies when baby is allowed unrestricted access to the breast. Yes, adding in chia seed, flax seed, oats, nuts and nut butters, and coconut water helps make milk. Certain people do better on certain herbs and foods because of how their specific body handles and processes food, vitamins, stress, hormones, and all of the other factors like anatomy and genetics. Finding a lactation consultant, peer counselor, or trained doula helps you look at your specific body and goals and helps you reach them. You can absolutely get there in your own, having someone counsel you through often gets you quicker results from their experience and wisdom. But the principle remains: emptying milk from the breast is the number one way to make breast milk.
Pumping while away from baby helps maintain your supply
Did you know that you will ALWAYS be able to make milk? You’ve had the milk making glands in your breasts since puberty. They’re like little empty clusters of balloons at the back of the breast. Pregnancy activates your milk making hormones, allowing the glands to expand and start filling with milk between 16-20 weeks gestation. In the early days after birth, the more stimulation the breast has (from feeding or pumping), the more the milk making glands and their corresponding hormone receptors multiply. The milk balloons fill and empty milk multiple times per feeding.
After at least 40 days of not expressing any milk, once you completely wean, your milk making balloons deflate and become dormant, like before pregnancy. But they aren’t dead. Pregnancy and breastfeeding hormones caused a permanent change in your body. Your milk making glands will FOREVER remember how to make milk. They can ALWAYS make milk again, no matter how long it has been. They just need enough of the right stimulation to turn on and start filling again. Some times years after breastfeeding a mother may feel the tingle of let down if she hears a baby cry. Or she may leak if her partner does enough nipple stimulation. There are grandmothers in other cultures who bring back milk to breastfeed their grandchildren! Our bodies are AMAZING!! Now you know!
What can cause a late onset decreased milk supply?
1.The mother is pregnant again. Milk supply decreases during pregnancy. Domperidone will not work when the mother is pregnant.
2.The mother is taking some hormonal birth control method (pill including progestin only pill, IUD, etc)
3.The mother is breastfeeding on only one side at a feeding or “block feeding” (several feedings in a row on the same breast, used to treat “overabundant milk ejection, “overabundant milk supply”). I have posted on “block feeding” previously.
4.Some medications other than hormones can decrease the milk supply (antihistamines for example).
5.Can an emotional shock decrease the milk supply? Possible but unusual in our experience.
6.Blocked ducts/mastitis as well as any febrile illness may decrease the milk supply.
7.The use of bottles more than occasionally can very much decrease the milk supply.
8.”Overdoing it”. It’s time that others do most of the usual chores that fall on women’s shoulders.
9.An “abundant milk supply” associated with a less than “ideal” latch. In this situation, the milk flows into the baby’s mouth with little participation of the baby. The baby may often choke while breastfeeding, especially when the mother has a milk ejection reflex. A tongue tie is a common cause of a baby having a less than “ideal” latch and can be a significant cause of late onset decreased milk supply even if neither the mother or the baby had problems early on.
This problem of late onset decreased milk supply and accompanying symptoms is typically the problem of the mother who once had an abundant milk supply and milk supply may still be quite good, but less than it once was.
How can I make fattier milk? I get this question a lot. Fat in breast milk changes constantly both throughout the day and as baby ages. It is predominantly influenced by how full/empty the breast is which tells your body how old your baby is. Newborns nurse around the clock and have a higher milk fat content than toddlers who may only nurse a handful of times a day and are getting their fats from table foods. Your diet does not usually have an effect on the quantity of fat present in breast milk but it can change the type- saturated, trans, monounsaturated, polyunsaturated.
I often get questions about foremilk/hindmilk as related to making a fattier milk. But what is fore milk/hindmilk? Is that even a thing? The breast only makes one type of milk, however, because of the way milk is released during a feeding, the fat content can change. Fats make up about 3-5% of the nutrients of breast milk and each ounce of contains about 1.2 grams of fat. Milk is made in the alveoli, which are grape-like clusters of cells at the back of the breast. Once the milk is made, it is squeezed out through the alveoli into the milk ducts, which resemble highways and carry the milk through the breast to the nipple. As milk is produced, fat globules in the milk stick to each other and to the walls of the milk ducts. As time passes, milk gradually moves toward the nipple as the breasts fill, pushing the thin watery milk forward while leaving the denser and fattier hindmilk behind (because the fat is sticking to the walls of the ducts). Shorter time between feedings or pumping a help keep the hind milk at the front of the breast. Think of it like turning on a faucet in the sink.
At first, the water comes out cold and then gradually gets warmer until it is hot. If you come back a minute later and turn the faucet on again, it will still be relatively warm. However, if wait an hour, the water will be cold. You’ll have to wait for it to warm up again. Breast milk fat is similar.
When the baby first latches on, the higher-water content foremilk is released. Little by little the milk becomes fattier as fat globules are pulled down from the ducts. Frequent feedings or pumping mean the milk doesn’t have time to “get cold.” There is no switch that gets flipped – the change from foremilk to hindmilk is gradual. There is less foremilk for your baby to go through before they get to the fattier milk. Basically, the less time in between feedings, the higher the fat content at the beginning of that particular feeding.
Here are the best strategies to help increase the fat in your milk:
📌Nurse or pump more frequently. The fullness of the breast makes the most difference with the amount of fat in your milk. The fuller the breast, the more water content is in your milk because your body thinks baby is dehydrated from going a long time without feeding or that you have an older baby that is getting fats from table foods. The shorter amount of time you go between feeding or pumping, the higher the fat content in your milk. You will see a smaller volume, but a higher fat content.
📌Drain the breast. Let your baby completely finish on one side before switching to the other side. Emptier breast’s have higher milk fat content.
📌Use your hands. Compressing and massaging the breast from the chest wall down toward the nipple while feeding and/or pumping helps push fat (made at the back of the breast in the ducts) down toward the nipple faster.
📌Eat more healthy, unsaturated fats, such as nuts, wild caught salmon, avocados, seeds, eggs, and olive oil.
📌 Increase your protein intake. This helps increase overall milk supply, which = more fat for your baby. Lean meats, chicken, fish, eggs, dairy, nuts, and seeds are the best dietary sources of protein. Vegetarians if you do not get enough protein from your food alone, consider adding a protein supplement in your routine.
📌Sunflower lethicin. Often used to relieve frequently blocked ducts, this supplement works by decreasing the stickiness of breast milk by mixing the fatty parts of breast milk with the watery parts to make it “slide out” easier. Some people believe that this helps increase the fatty acids in milk at the beginnings of feedings, too.
Switching baby too quickly from breast to breast while they are still actively sucking means that they aren’t getting enough time to let the fattier hindmilk unstick from the milk ducts.
TAKE AWAY:
Depending on your nursing pattern, it’s possible for fat content to be higher at the beginning of a particular feeding than it is at the end of other feedings. The longer the time between feedings, the lower the fat content at the beginning of the next feeding. If feedings are closer together, you’re starting off with a higher fat content.
Because every baby varies in the amount of time it takes him to receive his fill of the higher-fat milk at the end of the feeding, it’s important not to switch breasts while baby is actively nursing.